
https://wirepoints.org/ignorance-ab...rch-report-says-huge-age-variance-wirepoints/
Americans have been “blinded from science,” according to a recent research report about their understanding of COVID-19. And it’s not about the controversial aspects like treatments and lockdown policies. It’s about ignorance of fundamental, undisputed facts on who is at risk.
A leading financial firm, Franklin Templeton, figured that people’s behavioral response to the pandemic will play a crucial role in shaping the economic recovery, so they teamed up with Gallup, the polling outfit, to find out what people know and don’t know.
“These results are nothing short of stunning,” concluded the firm. “Six months into this pandemic, Americans still dramatically misunderstand the risk of dying from COVID-19.”
That’s no exaggeration, and the implications go far beyond the economic behavior Franklin Templeton was interested in.
Here is what they found:
First, the Franklin Templeton-Gallup survey found that the general population has little understanding how heavily the pandemic is focused on the older population. It is not broad-based. From the report:
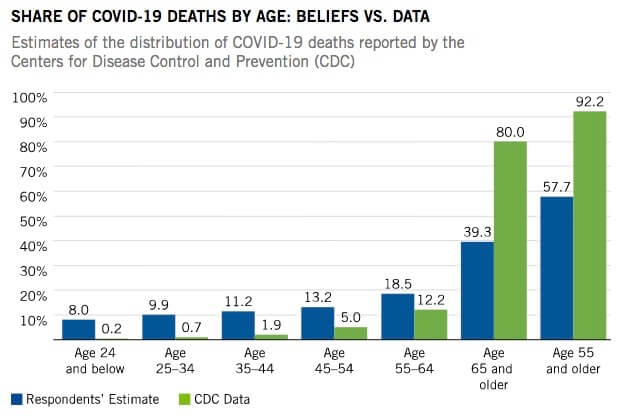
Source: They Blinded Us from Science, Franklin Templeton Report
In Illinois, too, coronavirus deaths are very heavily concentrated in the older population. The Franklin-Gallup survey about perceptions is not broken down by state, but we do have the underlying facts for Illinois.
The state’s data say 82% of COVID-19 death victims are 60 or older. Most Illinoisans undoubtedly don’t know that because only broad averages are normally reported. Many critics of lockdown policies, including Wirepoints, have long argued against one-size-fits all policies. Efforts, instead, should be more focused on those truly at risk – the elderly and those with comorbidities. We update our coronavirus data report every day that includes deaths by age group.
The lower your age the greater the ignorance:
What’s perhaps most striking from the survey is the connection between age of the respondents and their misconception about the virus. The younger you are, the more likely it is that you don’t understand.
“The discrepancy with the actual mortality data is staggering: for people aged 18–24, the share of those worried about serious health consequences is 400 times higher than the share of total COVID deaths; for those age 25–34 it is 90 times higher,” says the report. “The chart below truly is worth a thousand words:”
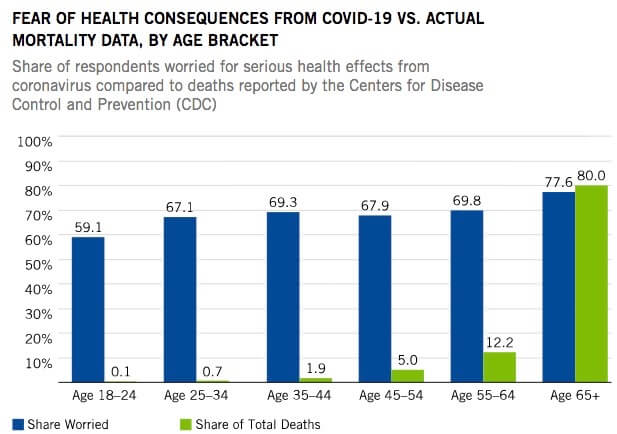
Source: They Blinded Us from Science, Franklin Templeton Report
The only good news there is that folks 65 and older are much more aware of the heightened risk for their own age group.
Social media and partisanship blamed:
The report blames the ignorance on two major culprits: the quality of information and the extreme politicization of the COVID-19 debate:
Fear and anger are the most reliable drivers of engagement; scary tales of young victims of the pandemic, intimating that we are all at risk of dying, quickly go viral; so do stories that blame everything on your political adversaries. Both social and traditional media have been churning out both types of narratives in order to generate more clicks and increase their audience.
The report found significant difference across partisan lines, though it did not include much neevidence:
According to our study, political affiliation is as powerful as age in predicting whether someone would be likely to eat at a restaurant indoors; Democrats have roughly the same willingness to eat in a restaurant at 25% capacity as Republicans do in a restaurant at full capacity. Individual risk from COVID-19 depends on age and health, but perceived risk depends on one’s politics— and it’s perceived risk that drives behavior. Conversely, previous Gallup research has found that Republicans have been less likely to accept public health guidelines like wearing a mask, regardless of the local rate of infection—again evidence that partisanship plays an important role.
Implications:
Whatever the causes, what’s clear from the study is that most Americans don’t understand COVID-19’s age discrimination. Risks are concentrated far more heavily on the older population than people think, especially young people.
One consequence for business people is that consumers are prepared to pay up for more security from the virus, according to the report. For example, it says, air travelers are willing to pay more to get an empty seat next to them.
But the implications go far beyond business considerations, as the report itself nicely concludes:
From a public interest perspective, we believe the top priority should be better information and a less partisan, more fact-based public debate. It is shocking that six months into the pandemic so many people still ignore the basic mortality statistics, with perceived risk driven by political leanings rather than individual age and health. Misperceptions of risk distort both individual behavior and policy decisions.
The fact that a large share of the population overestimates the COVID-19 danger to the young will make a targeted public health response more difficult to agree on. We think it is also likely to delay the recovery, causing a deeper and prolonged recession.
Amen to that.
*Mark Glennon is founder of Wirepoints.
Our additional articles and research on COVID-19 are here.
Americans have been “blinded from science,” according to a recent research report about their understanding of COVID-19. And it’s not about the controversial aspects like treatments and lockdown policies. It’s about ignorance of fundamental, undisputed facts on who is at risk.
A leading financial firm, Franklin Templeton, figured that people’s behavioral response to the pandemic will play a crucial role in shaping the economic recovery, so they teamed up with Gallup, the polling outfit, to find out what people know and don’t know.
“These results are nothing short of stunning,” concluded the firm. “Six months into this pandemic, Americans still dramatically misunderstand the risk of dying from COVID-19.”
That’s no exaggeration, and the implications go far beyond the economic behavior Franklin Templeton was interested in.
Here is what they found:
First, the Franklin Templeton-Gallup survey found that the general population has little understanding how heavily the pandemic is focused on the older population. It is not broad-based. From the report:
- On average, Americans believe that people aged 55 and older account for just over half of total COVID-19 deaths; the actual figure is 92%.
- Americans believe that people aged 44 and younger account for about 30% of total deaths; the actual figure is 2.7%.
- Americans overestimate the risk of death from COVID-19 for people aged 24 and younger by a factor of 50; and they think the risk for people aged 65 and older is half of what it actually is (40% vs 80%).
Source: They Blinded Us from Science, Franklin Templeton Report
In Illinois, too, coronavirus deaths are very heavily concentrated in the older population. The Franklin-Gallup survey about perceptions is not broken down by state, but we do have the underlying facts for Illinois.
The state’s data say 82% of COVID-19 death victims are 60 or older. Most Illinoisans undoubtedly don’t know that because only broad averages are normally reported. Many critics of lockdown policies, including Wirepoints, have long argued against one-size-fits all policies. Efforts, instead, should be more focused on those truly at risk – the elderly and those with comorbidities. We update our coronavirus data report every day that includes deaths by age group.
The lower your age the greater the ignorance:
What’s perhaps most striking from the survey is the connection between age of the respondents and their misconception about the virus. The younger you are, the more likely it is that you don’t understand.
“The discrepancy with the actual mortality data is staggering: for people aged 18–24, the share of those worried about serious health consequences is 400 times higher than the share of total COVID deaths; for those age 25–34 it is 90 times higher,” says the report. “The chart below truly is worth a thousand words:”
Source: They Blinded Us from Science, Franklin Templeton Report
The only good news there is that folks 65 and older are much more aware of the heightened risk for their own age group.
Social media and partisanship blamed:
The report blames the ignorance on two major culprits: the quality of information and the extreme politicization of the COVID-19 debate:
- People who get their information predominantly from social media have the most erroneous and distorted perception of risk.
- Those who identify as Democrats tend to mistakenly overstate the risk of death from COVID-19 for younger people much more than Republicans.
Fear and anger are the most reliable drivers of engagement; scary tales of young victims of the pandemic, intimating that we are all at risk of dying, quickly go viral; so do stories that blame everything on your political adversaries. Both social and traditional media have been churning out both types of narratives in order to generate more clicks and increase their audience.
The report found significant difference across partisan lines, though it did not include much neevidence:
According to our study, political affiliation is as powerful as age in predicting whether someone would be likely to eat at a restaurant indoors; Democrats have roughly the same willingness to eat in a restaurant at 25% capacity as Republicans do in a restaurant at full capacity. Individual risk from COVID-19 depends on age and health, but perceived risk depends on one’s politics— and it’s perceived risk that drives behavior. Conversely, previous Gallup research has found that Republicans have been less likely to accept public health guidelines like wearing a mask, regardless of the local rate of infection—again evidence that partisanship plays an important role.
Implications:
Whatever the causes, what’s clear from the study is that most Americans don’t understand COVID-19’s age discrimination. Risks are concentrated far more heavily on the older population than people think, especially young people.
One consequence for business people is that consumers are prepared to pay up for more security from the virus, according to the report. For example, it says, air travelers are willing to pay more to get an empty seat next to them.
But the implications go far beyond business considerations, as the report itself nicely concludes:
From a public interest perspective, we believe the top priority should be better information and a less partisan, more fact-based public debate. It is shocking that six months into the pandemic so many people still ignore the basic mortality statistics, with perceived risk driven by political leanings rather than individual age and health. Misperceptions of risk distort both individual behavior and policy decisions.
The fact that a large share of the population overestimates the COVID-19 danger to the young will make a targeted public health response more difficult to agree on. We think it is also likely to delay the recovery, causing a deeper and prolonged recession.
Amen to that.
*Mark Glennon is founder of Wirepoints.
Our additional articles and research on COVID-19 are here.
