You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
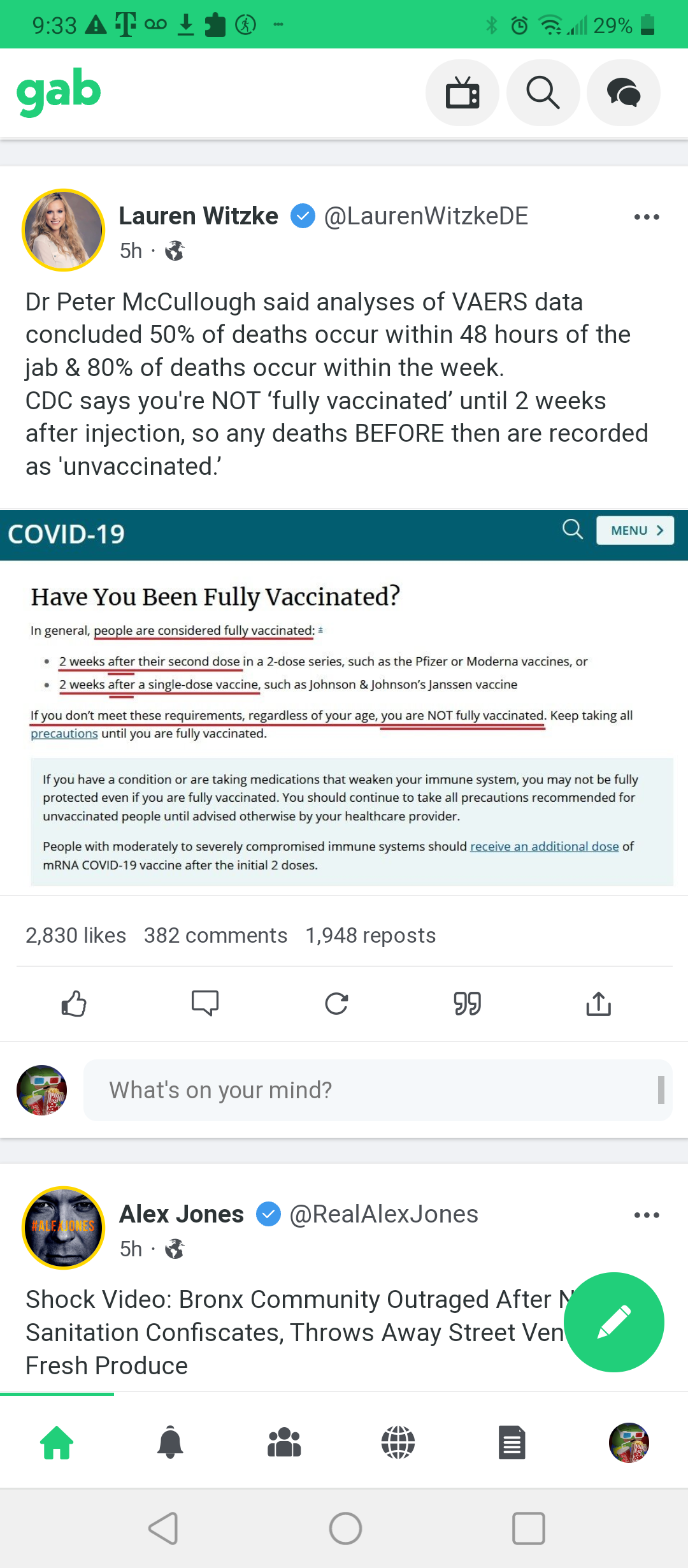
Check in if you're not getting the COVID "vaccine."
- Thread starter kcult
- Start date
- Replies 15,771
- Views 436,558
The War Wagon
Well-Known Member
Congratulations son - yo' momma's an IDIOT.

:quality(70)/d1hfln2sfez66z.cloudfront.net/09-25-2021/t_b03d115cbedb4bbf8662a95721a09c63_name_I_always_listen_to_my_mom_1stgrader_keep_614f497574d7d2649c192fcf_1_Sep_25_2021_16_34_33_poster.jpg)

The War Wagon
Well-Known Member
The Chinlees have OUR number, don't they?
1) Invent the disease
2) Get Mickey Mauci in on the deal
3) Help the demtards steal the election, for a senile old fool
4) Invent the... "cure." 🙄
5) March right in UN-impeded, when thesuckers Americans are incapacitated, or DEAD. 

1) Invent the disease
2) Get Mickey Mauci in on the deal
3) Help the demtards steal the election, for a senile old fool
4) Invent the... "cure." 🙄
5) March right in UN-impeded, when the
Last edited:
Fauci, Austin, Milley, and the rest of the Marxist Group fully known what is being reported by this doctor.
They are playing for the other team.
How do I know?
By their words? NO, by their actions, period.
Among the American Civilian population, some Ex-Military, The Marxist have solid support to FORCE our military to get the JAB as well. So, in this case of physically damaging and compromising America's Military Pilots, who among the Civilians are qualified for piloting & Flight Operations?
FWIW
I do not think "Micro-Soft Flight Simulator" counts, nor does flying a Drone bought At Wally Word.
AFFIDAVIT OF LTC. THERESA LONG M.D. IN SUPPORT OF A MOTION FOR A PRELIMINARY INJUNCTION ORDER
- a) None of the ordered Emergency Use Covid 19 vaccines can or will provide better immunity than an infection-recovered person;
- b) All three of the EUA Covid 19 vaccines (Comirnaty is not available), in the age group and fitness level of my patients, are more risky, harmful and dangerous than having no vaccine at all, whether a person is Covid recovered or facing a Covid 19 infection;
- c) Direct evidence exists and suggests that all persons who have received a Covid 19 Vaccine are damaged in their cardiovascular system in an irreparable and irrevocable manner;
- d) Due to the Spike protein production that is engineered into the user’s genome, each such recipient of the Covid 19 Vaccines already has micro clots in their cardiovascular system that present a danger to their health and safety;
- e) That such micro clots over time will become bigger clots by the very nature of the shape and composition of the Spike proteins being produced and said proteins are found throughout the user’s body, including the brain;
- f) That at the initial stage of this damage the micro clots can only be discovered by a biopsy or Magnetic Resonance Image (“MRI”) scan;
- g) That due to the fact that there is no functional myocardial screening currently being conducted, it is my professional opinion that substantial foreseen risks currently exist, which require proper screening of all flight crews.
- h) That, by virtue of their occupations, said flight crews present extraordinary risks to themselves and others given the equipment they operate, munitions carried thereon and areas of operation in close proximity to populated areas.
- i) That, without any current screening procedures in place, including any Aero Message (flight surgeon notice) relating to this demonstrable and identifiable risk, I must and will therefore ground all active flight personnel who received the vaccinations until such time as the causation of these serious systemic health risks can be more fully and adequately assessed.
- j) That, based on the DOD’s own protocols and studies, the only two valuable methodologies to adequately assess this risk are through MRI imaging or cardio biopsy which must be carried-out.
- k) That, in accordance with the foregoing, I hereby recommend to the Secretary of Defense that all pilots, crew and flight personnel in the military service who required hospitalization from injection or received any Covid 19 vaccination be grounded similarly for further dispositive assessment.
- l) That this Court should grant an immediate injunction to stop the further harm to all military personnel to protect the health and safety of our active duty, reservists and National Guard troops.
Ground our military pilots & flight crews
AFFIDAVIT OF LTC. THERESA LONG M.D. IN SUPPORT OF A MOTION FOR A PRELIMINARY INJUNCTION ORDER
Milley & Austin will get a promotion over this one.
Xi couldn't asked for a better plan

Stout
Thought Criminal
2A Bourbon Hound 2024
2A Bourbon Hound OG
Charter Member
Benefactor
Supporting Member
Multi-Factor Enabled
- Joined
- Dec 19, 2016
- Messages
- 18,263
12:20 then listen for a couple of minutes. He gives a good explanation for why you can't talk about all this with people who have been vaxxed.

Stout
Thought Criminal
2A Bourbon Hound 2024
2A Bourbon Hound OG
Charter Member
Benefactor
Supporting Member
Multi-Factor Enabled
- Joined
- Dec 19, 2016
- Messages
- 18,263

Jeremy Chardy: I regret getting vaccinated, I have series of problems now
Chardy insists he is unable to train and play after taking the jab.
 www.tennisworldusa.org
www.tennisworldusa.org
Former world No. 25 Jeremy Chardy says he has a "series of problems" after taking the COVID-19 vaccine and his 2021 season is over. This summer, 34-year-old Chardy decided to get vaccinated and it didn't work out well for him.
Chardy, now ranked at No. 73 in the world, claims he is unable to train and play. "Since I got my vaccine [between the Olympics and the US Open], I have a problem, I have a series of problems. As a result, I can't train, I can't play.
Stout
Thought Criminal
2A Bourbon Hound 2024
2A Bourbon Hound OG
Charter Member
Benefactor
Supporting Member
Multi-Factor Enabled
- Joined
- Dec 19, 2016
- Messages
- 18,263
I, Lieutenant Colonel Theresa Long, MD, MPH, FS being duly sworn, depose and state as follows:
1. I make this affidavit, as a whistle blower under the Military Whistleblower Protection Act, Title 10 U.S.C. § 1034, in support of the above referenced MOTION as expert testimony in support thereof.
2. The expert opinions expressed here are my own and arrived at from my persons, professional and educational experiences taken in context, where appropriate, by scientific data, publications, treatises, opinions, documents, reports and other information relevant to the subject matter and are not necessarily those of the Army or Department of Defense.
Experience & Credentials
3. I am competent to testify to the facts and matters set forth herein. A true and accurate copy of my curriculum vitae is attached hereto as Exhibit A.
4. After receiving a bachelor’s degree from the University of Texas Austin, completed my medical degree from the University of Texas Health Science Center at Houston Medical School in 2008. I served as a Field Surgeon for ten years and went on to complete a residency in Aerospace and Occupational Medicine at the United States Army School of Aviation Medicine, Fort Rucker, AL. I hold a Master’s in Public Health, and I have been trained by the Combat Readiness Center at Ft. Rucker as an Aviation Safety Officer. Additionally, I have trained in the Medical Management of Chemical and Biological Causalities at Fort Detrick and USAMIIRD.
5. I am board certified in flight Aerospace Medicine and board eligible in Occupational Medicine.
6. I am currently serving as the Brigade Surgeon for the 1st Aviation Brigade Ft. Rucker, Alabama and am responsible for certifying the health, mental and physical ability, and readiness for all nearly 4,000 individuals on flight status on this post.
7. My appended curriculum vitae further demonstrates my academic and scientific achievements by me over the past thirteen years.
8. Prior to the outset of the pandemic, I received specialized military training from Infectious Disease doctors from the Army, Navy and Air Force on emerging infectious disease threats, FEMA training, Emergency preparedness training, Medical effects of Ionizing Radiation, OSHA, Aerospace Toxicology, Epidemiology, Biostatistics, medical research and disaster planning. More recently I have functioned as a medical and scientific advisor to an Aviation training Brigade seeking to identify risk mitigation strategies, and bio statistical analysis of SARS- Cov-2 (“Covid 19”) infections in both vaccinated and unvaccinated Soldiers. In so doing, I have identified, diagnosed and treated Covid 19 pathogenic infections. I have observed vaccine adverse events following the administration of EUA vaccines, and followed the success of Soldiers who obtained various Covid 19 therapies outside the military. The majority of the service members within the DOD population are young and in good physical condition. Military aviators are a subset of the military population that has to meet the most stringent medical standards to be on flight status. The population of student pilots I take care of are primarily in their 20s-30s, males and in excellent physical condition. The risk of serious illness or death in this population from SARs-CoV-2 is minimal, with a survival rate of 99.997%.
9. In observing, studying and analyzing all the available data, information, samples, experiences, histories and results of these treatments and inoculations provided, I have formulated a professional opinion, which requires me to report those findings to superiors in the chain of command and colleagues in the military. I have done so with mixed results in terms of acceptance, rejection and threats of punishment for so sharing.
10. The application of risk management is critical to the safety and success in both medicine and aviation. Aerospace Medicine is a specialty devoted to safety of flight by the aeromedical dispositioning and treatment of flight crew members, as accomplished by the consistent and careful application of risk mitigation and management strategies. ATP 5-19, 1-3. Risk Management (RM)1 outlines a disciplined approach to express a risk level in terms readily understood at all echelons.
1 adminpubs.tradoc.army.mil/regulations/TR385-2withChange1.docx 4
Case 1:21-cv-02228-RM-STV Document 17 Filed 09/24/21 USDC Colorado Page 7 of 269
11. 1-6. States, “A risk decision is a commander, leader, or individual’s determination to accept or not accept. The risk(s) associated with an action he or she will take or will direct others to take. RM is only effective when specific information about hazards and risks is passed to the appropriate level of command for a risk decision. Subordinates must pass specific risk information up the chain of command.”
12. “When the specific information about hazards and risks is passed to the appropriate level of command for a risk decision. Subordinates must pass specific risk information up the chain of command. Conversely, the higher command must provide subordinates making risk decisions or implementing controls with the established risk tolerance—the level of risk the responsible commander is willing to accept. RM application must be inclusive; those executing an operation and those directing it participate in an integrated process”.
13. 1-7. States, “In the context of RM, a control is an action taken to eliminate a hazard or to reduce its risk. Commanders establish local policies and regulations if appropriate”.
14. The five steps of Risk management include; 1. Identify the hazards, 2. Assess the hazards, 3. Develop controls and make risk decisions, 4. Implement controls, 5. Supervise and evaluate.
15. It is therefore my responsibility and that of every leaders to apply the steps of risk management to the current pandemic and countermeasures used. The CDC and the FDA are civilian agencies that do not have the mission of National Defense that the DOD has. Guidance and recommendations made by these civilian agencies must be filtered through strategic perspective of national defense and the potential risks recommendations may have on the health of the entire fighting force. Ensuring that the health of the fighting force is not compromised is a strategic imperative, for which every military physician is responsible to of the entire fighting force. Ensuring that the health of the fighting force is not compromised is a strategic imperative, for which every military physician is responsible to ensure.
16. Step 1: Identify the hazards: As defined by FM 1-02.1 Operational Terms, pg. 1- 48, hazard is a condition with the potential to cause injury, illness, or death of personnel; damage to or loss of equipment or property; or mission degradation.
17. Step 2: Assess the Hazards: There are numerous therapeutic agents that have been proven to significantly reduce infection and therefore provide protection from the harmful effects of SARs-CoV-2.
18. Literature has demonstrated that natural immunity is durable, completed, and superior to vaccination immunity to SARs-CoV-2. mRNA vaccines produced by Pfizer and Moderna both have been linked to myocarditis, especially in young males between 16-24 years old,2 The majority of young new Army aviators are in their early twenties. We know there is a risk of myocarditis with each mRNA vaccination. We additionally now know that vaccination does not necessarily prevent infection or transmission of SARs-CoV-2Therefore individuals fully vaccinated with mRNA vaccines have at least two independent risk factors for myocarditis after vaccination. Additional boaster shots add more risk. It is impossible to perform a risk/benefit analysis on the use of mRNA as counter measures to SARs-CoV-2 without further data… Use of mRNA vaccines in our fighting force, presents a risk of undetermined magnitude, in a population in which less than 20 active-duty personnel out of 1.4 million, died of the underlying SARs- CoV-2.
19. Aircrew Training Program (ATP) 5-19, 1-8. Accept No Unnecessary Risk, states, “An unnecessary risk is any risk that, if taken, will not contribute meaningfully to mission accomplishment or will needlessly endanger lives or resources. Army leaders accept only a level of risk in which the potential benefit outweighs the potential loss.
20. Research shows that most individuals with myocarditis do not have any symptoms. Complications of myocarditis include dilated cardiomyopathy, arrhythmias, sudden cardiac death and carries a mortality rate of 20% at one year and 50% at 5 years. According to the National Center for Biotechnology Information, U.S. National Library of Medicine, “despite optimal medical management, overall mortality has not changed in the last 30 years”.
21. Step 3: Develop controls and make risk decisions: Because vaccination with mRNA increase the risk of myocarditis, a comprehensive screening program should be implemented immediately to identify individuals who have been affected and attempt to mitigate immediate risks and long-term disability.
22. Step 4: Implement Controls: Send out clear guidance to all DOD healthcare professionals on risks of-vaccination myocarditis. Compulsory SARs-CoV-2 mRNA vaccination program should be immediately suspended until research can be done to determine the true magnitude of risk of myocarditis in individuals who have been vaccinated. We must evaluate and immediately implement alternatives to mRNA vaccines, to include Ivermectin (FDA approved 1996), Remdesivir (FDA approved 2020), Hydroxychloroquine (FDA approved 1955), Regeneron (FDA EU approved 2020). Review VAERS data for deaths from COVID for age-matched data and data from active duty COVID deaths within the DOD to perform a risk/benefit analysis.
23. Step 5: Supervise and evaluate: We must establish a screening program to identify those at increased risk of myocarditis, i.e. those that have, received mRNA vaccinations with Comirnaty, BioNTech or Moderna, or have any of the following symptoms chest pain, shortness of breath or palpitations They should have screening tested performed in accordance with the CDC recommendations prior to return to flight duties. Per the CDC guidelines the initial evaluation of individuals identified according to the above criteria include; ECG, troponion level, inflammatory markers such as the C-reactive protein and erythrocyte sedimentation rate. It should be noted that the gold standard for diagnosis of myocarditis is end myocardial biopsy (EMB).
24. Given that the labels for Comirnaty and BioNtech clearly state that the vaccination should not be given to individuals that are allergic to ingredients. I have noted that one of the primary ingredients of the Lipid Nanoparticle delivery system is “ALC 1035” (two attachments, parts highlighted) in the Pfizer shots. The forth attachment is the toxicity report on ALC-1035, which comprises between 30-50% of the total ingredients.3 The Safety Data Sheet, (attached as Exhibit B) for this primary ingredient states that it is Category 2 under the OSHA HCS regulations (21 CFR 1910) and includes several concerning warnings, including but not limited to:
- Seek medical attention if it comes into contact with your skin;
- If inhaled and If breathing is difficult, give cardiopulmonary resuscitation
- Evacuate if there is an environmental spill
- the chemical, physical, and toxicological properties have not been completely investigated
- Caution: Product has not been fully validated for medical applications. For research use only
26. As such, I believe it is reasonable to conclude that many humans are allergic to these dangerous and deadly toxins and therefore should not take vaccinations with either Comirnaty or BioNtech. Again, I have identified an agent that possess a significant hazard to Soldiers, which would fall under DA Pam 385-61 Toxic Safety Standards cited in 2-11.
27. My assessment is that ALC 0315 is a known toxin with little study, specifically restricted to “research only“ and effectively has no prior use history, with the SDS designation of (GHS02), listed as H315 and H319, in other words, hazardous if inhaled, ingested or in contact with skin and a health hazard with the designation (P313). A review of the SDS outlines that it is not for human or veterinary use,
28. I have not taken significant time to delineate the risks of other Covid 19 Vaccines other than the Safety Data Sheet of Moderna’s key ingredient, SM-102 (attached as Exhibit C). Suffice it to say that SM-102 is significantly more dangerous than the Pfizer ALC 3015 and it appears that the DOD is not actively acquiring or distributing this IND/EUA. If the DOD were to undertake use of the Moderna vaccine, one can expect a much higher Serious Adverse Event and fatality rate given that SM-102 carries an express warning “Skull and Crossbones” characterized under the GHS06 and GHS08. In other words, this Moderna ingredient is deadly.
29. Given that these Covid 19 Vaccines were both Investigational New Drugs and Emergency Use Authorization vaccines, I have taken considerable time to understand potential risks, hazards and dangers these and any new drug or Investigational New Drug will may have on the health, safety and operational readiness or ability of pilots under my care and at this post. I have sought to research military records and track systems for recording events and Serious Adverse Events and fatalities associated with vaccines, new vaccines and Emergency Use, investigational vaccines in computer data systems recommended by the General Accounting Office in 2002 and ordered to be developed and implemented by the Secretary of Defense in 2003.
30. A weekly MEDSITREP report fails to report the CDC data from VAERS or internal data regarding vaccine adverse events. Despite recommendation made by the Government Accountability Office in the GAO’s survey of Guard and Reserve Pilots and Aircrew GAO-02-445, published Sep 20,2002, in which it was recommended that the Secretary of Defense should direct the establishment of an active surveillance program (unlike the passive VAERS) to identify and monitor adverse events, was not implemented. I have been unable to locate, access or asses any data, data base or internal system to track, store, evaluate or research the effects of vaccines on our military members or pilots.
31. I have also reviewed scientific data and peer reviewed studies that discuss, analyze results and conclude that natural immunity is at least as good if not far superior to any Covid Vaccine available at this time. I have also reviewed Dr. Peter McCullough’s sworn affidavit in support of and in relation to the Complaint filed in this case and have reviewed its supporting data. An additional peer-reviewed study not referenced in Dr. McCullough’s materials also supports the same conclusions drawn and reports that natural immunity provides a 13 fold better protection against Covid 19 infections than any currently available Covid 19 Vaccine6. More recently, in a meeting of the FDA Advisory Committee on September 17 of this year, fourteen of seventeen members voted against the authorization of any Covid booster vaccines in the juvenile age group having noted that the vaccine program has breached the defining test under the EUA statute as to whether the experimental treatment benefits outweigh the risks; in fact, they found the shots are far more dangerous than helpful in this age group and some voiced concerns that this would apply generally to all age groups.7
32. I am also aware of the Secretary of Defense Austin’s order in relation to Covid Vaccine mandates made this week. In an information paper, it was stated that, “Unit personnel should use only as much force as necessary to assist medical personnel with immunizations.” The use of force to administer a medical treatment or therapy against the will of a mentally competent individual constitutes medical battery and universally violates medical ethics. Currently, I am not aware of the Comirnaty available within the DOD. Emergency Use Authorized vaccines, despite the attempt to characterize some of them as approved despite such approved versions not being available and regardless of a military member’s prior immunity to Covid 19; even where it may be demonstrated with a recent antibody test.
33. Finally, I have reviewed a recent study entitled “US COVID-19 Vaccines Proven to Cause More Harm than Good Based on Pivotal Clinical Trial Data Analyzed Using the Proper Scientific Endpoint, All Cause Severe Morbidity,” by J. Bart Classen, MD and published in Trends in Internal Medicine; August 25, 2021. Attached as Exhibit D.
34. I have also seen policies, memoranda and guidance as it relates to exemptions for vaccinations as fully detailed in Army Regulation 40-562, which purport to eliminate any exemption for prior immunity by our military personnel.
Opinion
35. I have reviewed the Motion for a Preliminary Injunction which discusses the issue
of prior immunity benefits outweighing the risks of using experimental Covid 19
Vaccines, together with proposed exhibits and materials cited therein. In opinion on this subject matter, I am also drawing my own conclusions that will be put into practice in my current role as an Army flight surgeon knowing full well the horrific repercussions this decision may befall me in terms of my career, my relationships and life as an Army doctor.
36. I personally observed the most physically fit female Soldier I have seen in over 20 years in the Army, go from Colligate level athlete training for Ranger School, to being physically debilitated with cardiac problems, newly diagnosed pituitary brain tumor, thyroid dysfunction within weeks of getting vaccinated. Several military physicians have shared with me their firsthand experience with a significant increase in the number of young Soldiers with migraines, menstrual irregularities, cancer, suspected myocarditis and reporting cardiac symptoms after vaccination. Numerous Soldiers and DOD civilians have told me of how they were sick, bed-ridden, debilitated, and unable to work for days to weeks after vaccination. I have also recently reviewed three flight crew members’ medical records, all of which presented with both significant and aggressive systemic health issues. Today I received word of one fatality and two ICU cases on Fort Hood; the deceased was an Army pilot who could have been flying at the time. All three pulmonary embolism events happened within 48 hours of their vaccination. I cannot attribute this result to anything other than the Covid 19 vaccines as the source of these events. Each person was in top physical condition before the inoculation and each suffered the event within 2 days post vaccination. Correlation by itself does not equal causation, however, significant causal patterns do exist that raise correlation into a probable cause; and the burden to prove otherwise falls on the authorities such as the CDC, FDA, and pharmaceutical manufacturers. I find the illnesses, injuries and fatalities observed to be the proximate and causal effect of the Covid 19 vaccinations.
38. I can report of knowing over fifteen military physicians and healthcare providers who have shared experiences of having their safety concerns ignored and being ostracized for expressing or reporting safety concerns as they relate to COVID vaccinations. The politicization of SARs-CoV-2, treatments and vaccination strategies have completely compromised long-standing safety mechanisms, open and honest dialogue, and the trust of our service members in their health system and healthcare providers.
39. The subject matter of this Motion for a Preliminary Injunction and its devastating effects on members of the military compel me to conclude and conduct accordingly as follows:
- a) None of the ordered Emergency Use Covid 19 vaccines can or will provide better immunity than an infection-recovered person;
- b) All three of the EUA Covid 19 vaccines (Comirnaty is not available), in the age group and fitness level of my patients, are more risky, harmful and dangerous than having no vaccine at all, whether a person is Covid recovered or facing a Covid 19 infection;
- c) Direct evidence exists and suggests that all persons who have received a Covid 19 Vaccine are damaged in their cardiovascular system in an irreparable and irrevocable manner;
- d) Due to the Spike protein production that is engineered into the user’s genome, each such recipient of the Covid 19 Vaccines already has micro clots in their cardiovascular system that present a danger to their health and safety;
- e) That such micro clots over time will become bigger clots by the very nature of the shape and composition of the Spike proteins being produced and said proteins are found throughout the user’s body, including the brain;
- f) That at the initial stage of this damage the micro clots can only be discovered by a biopsy or Magnetic Resonance Image (“MRI”) scan;
- g) That due to the fact that there is no functional myocardial screening currently being conducted, it is my professional opinion that substantial foreseen risks currently exist, which require proper screening of all flight crews.
- h) That, by virtue of their occupations, said flight crews present extraordinary risks to themselves and others given the equipment they operate, munitions carried thereon and areas of operation in close proximity to populated areas.
- i) That, without any current screening procedures in place, including any Aero Message (flight surgeon notice) relating to this demonstrable and identifiable risk, I must and will therefore ground all active flight personnel who received the vaccinations until such time as the causation of these serious systemic health risks can be more fully and adequately assessed.
- j) That, based on the DOD’s own protocols and studies, the only two valuable methodologies to adequately assess this risk are through MRI imaging or cardio biopsy which must be carried-out.
- k) That, in accordance with the foregoing, I hereby recommend to the Secretary of Defense that all pilots, crew and flight personnel in the military service who required hospitalization from injection or received any Covid 19 vaccination be grounded similarly for further dispositive assessment.
- l) That this Court should grant an immediate injunction to stop the further harm to all military personnel to protect the health and safety of our active duty, reservists and National Guard troops.
41 As an Aerospace Medicine Specialist, and flight surgeon responsible for the lives of our Army pilots, I confirm and attest to the accuracy and truthfulness of my foregoing statements, analysis and attachments or references hereto:
_______________/S/__________________ LTC Theresa Long, MD, MPH, FS
I, Lieutenant Colonel Theresa Long, MD, MPH, FS, declare under the penalty of perjury of the laws of the United States of America, and state upon personal knowledge that:
Of course. Any why do you think that our overlords and illegal aliens are not mandated the shot?I just watched "Children of Men" all the way through, which I haven't done in close to ten years, I'm reckoning. In LIGHT of that, the Chinaflu jab, suddenly makes a LOT more sense! Population control... except amongst the immigrants, who DON'T get the jab.
ANYONE notice how the mohammedans had taken over London (not that they haven't ALREADY) in the movie. GUESS who's REALLY coming to dinner... WITHOUT the jab, here in 'MURICA? 🤨
GUESS who's gonna replace our low - & soon to be STERILE - birthrate here?
THEY ARE REPLACING US AND AMERICANS ARE TOO STUPID TO SEE IT.

Do Vaccinated Pregnant Women in Their First or Second Trimester have an 81.8% Chance of Miscarriage?
Guest Post by Martin Armstrong You have to wonder why universities are suddenly investigating if the vaccines are causing abortions. The government appears to have been playing around with the numb…
www.theburningplatform.com
Stout
Thought Criminal
2A Bourbon Hound 2024
2A Bourbon Hound OG
Charter Member
Benefactor
Supporting Member
Multi-Factor Enabled
- Joined
- Dec 19, 2016
- Messages
- 18,263
News Briefs – 09/26/2021 | Anonymous Conservative
www.anonymousconservative.com
French doctor arrested, dragged out of his home for prescribing Ivermectin to Covid patients.
New York preparing to enact a State of Emergency as the vaccine mandate creates hospital staff shortages. The governor’s solution is to fire all the hospital staff who won’t take the vaccine, and open up hiring to people with no certifications, retired people who haven’t practiced for some time, and uncertified foreigners who she will import to fill the roles. Notice, all of a sudden, Cabal can get its people hired, even if they normally couldn’t get hired. If you were looking to infiltrate agents into positions where they could kill with impunity, it might look like this.
From this Army Flight Surgeon’s affidavit:
Singapore is back in lockdown despite 80+% vaccinated as COVID-19 cases are at a record high.I personally observed the most physically fit female Soldier I have seen in over 20 years in the Army, go from Colligate level athlete training for Ranger School, to being physically debilitated with cardiac problems, newly diagnosed pituitary brain tumor, thyroid dysfunction within weeks of getting vaccinated. Several military physicians have shared with me their firsthand experience with a significant increase in the number of young Soldiers with migraines, menstrual irregularities, cancer, suspected myocarditis and reporting cardiac symptoms after vaccination. Numerous Soldiers and DOD civilians have told me of how they were sick, bed-ridden, debilitated, and unable to work for days to weeks after vaccination. I have also recently reviewed three flight crew members’ medical records, all of which presented with both significant and aggressive systemic health issues. Today I received word of one fatality and two ICU cases on Fort Hood; the deceased was an Army pilot who could have been flying at the time. All three pulmonary embolism events happened within 48 hours of their vaccination.
Florida COVID cases see a massive drop for the third consecutive week.
JustKeepSwimming
AKA dingleberry
2A Bourbon Hound 2024
2A Bourbon Hound OG
Charter Life Member
Benefactor
Supporting Member
Multi-Factor Enabled


They are going to need to add the jab deaths to there unfortunately.

Wait til Sars-1 gets reintroduced, weaponized MERs.
Stout
Thought Criminal
2A Bourbon Hound 2024
2A Bourbon Hound OG
Charter Member
Benefactor
Supporting Member
Multi-Factor Enabled
- Joined
- Dec 19, 2016
- Messages
- 18,263
Once Upon A Time...
<p>... <em>in a not-so-tiny nation called Spain, a nursing home had a nasty virus get into it.</em></p><p>It was March of 2020. The nasty virus was called Covid-19. And this nursing home,
market-ticker.org
Once Upon A Time...*
... in a not-so-tiny nation called Spain, a nursing home had a nasty virus get into it.
It was March of 2020. The nasty virus was called Covid-19. And this nursing home, like so many others all over the world, was full of elderly, morbid people. The mean age of residents was 85 and 48% were over 80 years old. It was a killing field, like so many others.....
Within three months 100% of the residents had caught the virus. Not presumed to have -- proved to have.
How do we know this? Because almost every one of them seroconverted. All but three out of 84 of them, to be precise.
Think about that last sentence for a second.
Almost every one of them seroconverted.
How's that possible? Many of them died, right? You can't seroconvert if you're dead.
No. Not only did nearly none die none went to the hospital either because they rapidly figured out how to stop the virus from killing people -- and did exactly that.
You would have thought this would have been all over the news. In point of fact not one mention of it was made. Further, not one write-up was made in medical journals either until January of 2021, which I missed. My bad -- out of the several hundred medical journal pieces, I missed this one. It was brought to my attention on my forum and my jaw immediately hit the floor.
The jab train must continue, you see. So must the ventilator train. So must the money train, the mask train and the rest of the BS we have endured for the last 18+ months.
So must the slaughter for money, the fear, and the lies.
So what did these few nursing homes do that nobody has done since and nobody reported out at the time?
Ed 9/25 11:30 - Reformatted the cut section; it got mangled by the forum. Still not what I'd like in terms of formatting, but at least it's readable now... and one typo corrected.1. Early start of treatment, regardless of the severity of patient symptoms.
- Antihistamines every 12 h: dexchlorpheniramine 2 mg, cetirizine 10 mg or loratadine 10 mg.
2. Patients with mild or recent-onset symptoms (cough, fever, general malaise, anosmia, polymyalgia):
- Azithromycin 500 mg orally every 24 h for 3 days if there is rapid improvement, and for 6 days if the duration of symptoms is prolonged.
- If pain or fever, acetaminophen 650 mg/6–8 h.
- Nasal washing and gargling with sodium bicarbonate water (half a glass of warm water with half a teaspoon of sodium bicarbonate).
3. If symptoms of severity (dyspnea, breathing difficulty, mild or moderate chest pain, with SpO2 <80%, heart rate >100 beats per minute at any time of the process):
- Antihistamines + Azithromycin (see mild treatment management)
- Levofloxacin 500 mg/12 h, up to 14 days of antibiotic treatment from diagnosis.
- Mepifilin solution, 50 mg/8 h as a bronchodilator, until subjective improvement. Patients with previous lung disease (asthma or COPD) used their usual bronchodilators.
- If the patient experienced increased breathing difficulty, prednisone 1 mg/kg/day divided into two doses until clinical improvement, and then it was slowly tapered down.
4. Prophylactic treatment for close contacts, including all asymptomatic residents:
- Antihistamines at the same dose as symptomatic patients.
Look at that top line.
Cetrizine is otherwise known as Zyrtec. Loratadine is otherwise known as Claritin. Dexchlorpheniramine is not often-used in the US anymore, but it used to be. The other two core drugs were Azithromycin and Levofloxacin, both common antibiotics with the first being the infamous "Zpak" from the HCQ+Zinc+Zpak combination that a fraudulent study was used to discredit.
Both of the first two antihistamines are available over the counter in most nations including the United States. The dosing they used is twice that on the label. The two antibiotics are both available anywhere for little money.
Before they started treating people three residents died. The entire group of them had the common maladies of old age -- hypertension, diabetes, COPD, cardiovascular disease. Most were using a huge range of existing drugs for their conditions (5 or more.)
As soon as they started treating people the following happened:
Not one adverse event occurred among these residents and staff and no hospitalizations were necessary either.All of our patients evolved satisfactorily and were recovered at the beginning of June. No adverse effects were recorded in any patient and no one required hospital admission. At the end of June, 100% of the residents and almost half of the workers had positive serology for COVID-19, most of them with past infection.
In pooled data 28% of the residents in similar nursing homes over the same time period died. In these two, once they started treating with cheap drugs, leading with those available over the counter in the US, ZERO -- I repeat -- ZERO had a bad reaction to the protocol, ZERO died and ZERO were admitted to a hospital for treatment.
ZERO.
It was one hundred percent effective.
Yes, it's a small sample. Go do the statistical math on the CI for that size sample and results if you insist.
Nobody cared.According to the mechanisms of action described, these drugs would act synergistically in the early stages of the disease, which is why we consider it essential to start the treatment as soon as possible. Once the virus has colonized the respiratory system, the effectiveness is probably more limited, and hence the failure of these treatments in more advanced stages of the disease, when hospital admission is necessary. In our experience, early double antibiotics were effective to control the process in cases with moderate symptoms.
Nobody reported on this.
Nobody duplicated it either.
I didn't even realize this study existed; had I known of it guess what I would have added to my protocol when I got Covid-19 the first week of August of this year, since it happens to be in my medicine cabinet already for seasonal allergies? Uh huh. Two 60ct bottles of generic Claritin equivalent costs about $12 at WalMart.
Folks, think about this long and hard: In the worst-case scenario for those who this virus should have killed -- it killed nobody. It should be killing statistically nobody today -- right here, right now. How to prevent it from doing so was discovered in March and April of 2020 and intentionally ignored worldwide.
It is still being ignored today.
With these numbers there is no reason to fear a Covid-19 infection. There is no reason to take a vaccine. There was never a reason to develop a vaccine, especially the ones we have today; infection that does not produce severe disease is sterilizing and thus wildly superior to vaccinated immunity which is now proved to be failing worldwide. There is no reason to wear a mask.
Every single one of these residents seroconverted and became immune with mild or moderate symptoms consistent with seasonal colds and flus and not one of them was put into the hospital or killed. The treatment is so ******ned cheap and available there's no excuse to not use it instantly on suspicion of infection and prophylactically among everyone else in your household at first sign of trouble.
You think the entire load of BS around HCQ and Ivermectin is bad? This is a thousand times worse.
Stout
Thought Criminal
2A Bourbon Hound 2024
2A Bourbon Hound OG
Charter Member
Benefactor
Supporting Member
Multi-Factor Enabled
- Joined
- Dec 19, 2016
- Messages
- 18,263
So, Are They Trying To Kill You or Are They Just Corrupt, Avaricious, and Stupid? - LewRockwell
Governments [and their bureaucracies] lie. They lie all the time. If they told people the truth, they wouldn’t last very long. –Legendary historian Dr. Howard Zinn We know from this meticulous independent analysis of Israeli Government health data that someone who gets the Pfizer mRNA jab is...
 www.lewrockwell.com
www.lewrockwell.com
We know from this meticulous independent analysis of Israeli Government health data that someone who gets the Pfizer mRNA jab is 14.6 times more likely to die in the next weeks than someone in a statistically matched group who doesn’t get jabbed. That’s 14.6 times more likely to die per day.
That means the mRNA jabs would have to protect you 100% from COVID death for nearly three years for them to be a break-even proposition. You know the jabs don’t protect you for three years because they’re already telling you you need to risk another jab and it hasn’t even been one year.
But it’s worse than that. This analysis doesn’t include the many vaccine side-effects because the official Israeli records don’t include them. While many of these side-effects may not kill you, they may leave you crippled in various ways and mark you for life. Bell’s Palsey, Guilian Barr Syndrome, stroke, heart inflamation, etc. for just a few examples.
And what happens after those dangerous initial weeks?
We don’t know for sure because there aren’t even those meticulous Israeli Government vaccine-related death records after that initial period.
We can, however, get a pretty good idea from the VAERS (Vaccine Adverse Event Reporting System) and equivalent EURO data bases where some — best estimate, only about 10% — of the vaccine related deaths and side-effects are reported. Even that meager 10% reported through VAERS alone shows completely unprecedented levels of vaccine related injury and death – – –
VAERS data released Friday [August 24, 2021] by the CDC showed a total of 623,343 reports of adverse events from all age groups following COVID vaccines, including 13,627 deaths [an increase of 559 over the data released last week] and 84,466 serious injuries [up 3,416 compared with the previous week] between Dec. 14, 2020 and Aug. 20, 2021. –COVID Vaccine Injury Reports Jump by 27,000 in One Week
Based on the VAERS 10% factor, those figures imply 6,233,430 adverse vaccine events, 844,660 serious injuries and 136,270 deaths. So far.
So, even though seriously underestimated, both VAERS and the EU verson reveal an unprecedented — but still only short-term — continuation of jab-related death and serious — often incurable — side-effects and injuries.
Unfortunately, the really long-term negative effects can’t be detected, verified, and analyzed because those require long-term tracking and verification.
How long-term is “long-term?”
In general, because of the major potential harm vaccines can do when widely administered, the normal “long-term” necessary to collect, verify, and analyze vaccine data is about six years but may be as long as 12 years. That means a minimum of six years of long-term data are required before a vaccine’s safety can be legitimately certified.
And keep in mind, such vaccine safety approval is actually a rare event. About 78% of experimental vaccines don’t make the grade.
Do we have six years of long-term data on the mRNA jabs?
So, have they been LEGITIMATELY certified “safe?”
OK, so they’re still “experimental,” regardless of FDA shenanigans.
So, first iteration, “Are They TRYING to Kill You or Are They Just Corrupt and Stupid?”
Either way, that means we’re likely in for some unpleasant surprises in the next five years and possibly many more years to come.
What sorts of “unpleasant surprises?”
There are at least two longer-term problems caused by the experimental mRNA vaccines — Pfizer, Moderna, AstraZenica, J&J, etc. — predicted by virologists, for which there is significant and developing data — and another problem that’s a lot more unpleasant. There may be others.
The first problem is what’s being called “the leaky vaccine” problem. Since their true efficacy has been lowered from the fake P.R. mid 90% range to a current low in the 30% “leaky” range, these mRNA jabs turn vaccinated folks into factories producing new mutated versions of COVID. This explains the rapid development of Delta, Mu, etc.
The second problem is called antiboddy dependent enhancement or ADE. ADE may cause mRNA vaccinated folks to have much more serious disease when later exposed to the actual COVID virus, especially if it’s a variant.
Further, this research shows that vaccinated folks may be overrun with virus, carrying 251 times as much virus as unvaccinated folks, and thus have the potential to become so-called “super-spreaders.”
But there’s a third problem, apparently unique to mRNA, which has caused animal tests — waived for the mRNA COVID vaccines — to fail. The animal subjects died of a plethora of causes, and may have been rendered incapable of reproduction.
It’s like this – – –
The mRNA jabs program your own cells to produce toxic COVID spike protein. They were specifically designed to do that. It’s these self-produced spike proteins that cause your immune system to produce antibodies.
But these experimental “vaccines” don’t always stay in your deltoid muscle — the usual injection site — like they’re supposed to. They circulate throughout your body, causing cells in many locations to produce the toxic COVID “spike protein.”
According to one Canadian doctor, this happened in 62% of his mRNA vaccinated patients.
But just like the original, the escaped toxic self-produced spike proteins damage cells in many organs — especially in the circulatory system — throughout the body, doing often irreversible micro-damage.
This explains the increased occurrence of circulatory problems like heart inflamation in mRNA vaccinated young men. It would in fact explain the wide range of effects of both COVID itself — and mRNA vaccine side-effects.
The problem is that the circulatory system produces micro-clots in response to the spike-induced cell damage. In many organs, the spike-caused damage doesn’t heal and the clots may block capillaries, thus starving parts of various organs of oxygen. For example, if in the brain, this would cause micro-strokes.
This sort of spike and micro-clot damage is very difficult to diagnose because, well, it’s micro. So far there’s only one test, normally used to diagnose large clots but it works even if there are a bunch of smaller clots as well.
That test is called the D-DIMER test, and if you’ve had the jab or know someone who has, and are having weird symptoms — often written-off as psychological — push for the D-DIMER test.
You can find more information on this long-term micro-clot syndrome here, here, and here, and especially here. They’re beginning to call it “vaccine-induced immune thrombotic thrombocytopenia” or VITT.
But we only know about some — and only some — of these mRNA-caused problems because every once-in-awhile, one of them manages to escape the establishment’s vaccine-protective cone-of-silence and then also manages to avoid the rampant media/internet censorship and character assassinations.
To get a clear picture of the net benefit of risking an mRNA jab, any ill-effects during that six-year period must be discovered, analyzed, quantified, and added to the 14.6x death-risk danger which only covers the deaths — not the other side-effects — during the tracked period immediately after the jab(s).
Further, the additional deaths, maimings, etc. only show up in longitudinal studies conducted over time, normally at least six years for vaccines remember. But we don’t have the six-year long-range experience and data to recognize and analyze those long-term effects. The medical establishment is just beginning to react to the clot dangers for example.
So it’s clear, Mr. Biden has it backwards. Given that the leaky vaccines propagate mutated variants, that ADE makes the vaccinated more susceptible to variants and getting seriously ill, and that vaccinated folks have a lot more virus in their nasal cavities and may become “super spreaders,” we don’t need to “protect the vaccinated from the unvaccinated.” The question is, “how do we protect the unvaccinated — in fact everyone — from the vaccinated?”
But even if the experimental mRNA vaccines were safe and effective — we now know they’re neither — there are still at least three reasons not to get jabbed with them anyway.
FIRST: For nearly everyone under the age of 60, COVID itself is of very little rational concern, less concern than seasonal flu for example — especially when measured against the dangers and expense of the jab. This is spectacularly true for children who hardly ever contract it — and the very few who do almost never die from it. And despite the outlandish media fear-mongering, children don’t pass it on to grandpa.
SECOND: There are extremely effective non-vaccine treatment alternatives with long track records of safety. According to their own rules, that means the F.D.A. is not permitted to grant emergency status to untested vaccines. Of course they did anyway. Afterall, if we’ve learned anything in the last year-and-a half, it’s that the rules only apply to us, not to them.
THIRD: We also know that natural immunity is at least 13 times more effective at stopping COVID-19 and it’s spread than the jab and yet the health bureaucracy and industry wants to vaccinate those with natural immunity anyway — including the kids — despite the 14.6x-plus death-danger from the vaccine.
Why? Do they want to kill you or are they just stupid? Or is there more to it? Are they avaricious? Is it the money?
The real tell is that whoever’s calling the shots on this farce is CENSORING everyone who calls attention to their numerous mistakes, misprints, unintended bias, fudges, fibs, misrepresentations, outright lies, fraud, etc. Some folks call such checking, testing, analyzing — and taking the time to do it — “Due Process of Science.”
NOTE TO DR. FAUCI: Without Due Process, you can’t claim it’s science.
And they’re censoring everyone from Dr. Robert Malone, who developed the mRNA technology used in these “vaccines” while he was working at the Salk Institute of Virology, to progressive star Dr. Naomi Wolf who’s been trying to warn us for over a year. And nearly everyone in between.
In the good old days, resorting to censorship was the kiss of death. The censorship itself was taken as prima facie proof the censor couldn’t rationally deal with challenges and was, well, just completely full of it.
You can draw your own conclusions.
So, are they trying to kill you or are they just corrupt, avaricious and stupid?
Trying to kill you?
Well, some thoughtful folks are trying to make that case. Here are three examples – – –
Why Are Globalists And Governments So Desperate For 100% Vaccination Rates? By Brandon Smith
The Conspiracy Theorists Were Right; It IS a “Poison-Death Shot”, Mike Whitney, The Unz Review
A Final Warning To Humanity From Former Pfizer Chief Scientist Michael Yeadon
That’s why the bottom line is, Are They TRYING to Kill You or Are They Just Corrupt, Avaricious and Stupid?
What do YOU think?
HERE for updates, additions, comments, and corrections.
AND, “Like,” “Tweet,” and otherwise, pass this along!
The Best of L. Reichard White

Stout
Thought Criminal
2A Bourbon Hound 2024
2A Bourbon Hound OG
Charter Member
Benefactor
Supporting Member
Multi-Factor Enabled
- Joined
- Dec 19, 2016
- Messages
- 18,263

The Jab That Broke The Camel's Back: Thousands Protest in Tel Aviv Over Israel's Vaccine Passport That Now Requires Citizens to Take Booster Shot to Be Considered "Fully Vaccinated" - (Video) | The Gateway Pundit | by Julian Conradson
At the end of last month, Israeli Health Officials announced that any individual who has not received a 3rd Jab within 6 months of their second dose would no longer be considered “fully vaccinated” under the countries vaccine passport system.

Stout
Thought Criminal
2A Bourbon Hound 2024
2A Bourbon Hound OG
Charter Member
Benefactor
Supporting Member
Multi-Factor Enabled
- Joined
- Dec 19, 2016
- Messages
- 18,263
- "The most difficult subjects can be explained to the most slow-witted man if he has not formed any idea of them already; but the simplest thing cannot be made clear to the most intelligent man if he is firmly persuaded that he knows already, without a shadow of doubt, what is laid before him." - The Kingdom of God Is Within You (1894)
And Australia is at 7 so let that sink in...

Why are the FDA and CDC advisory panel members so afraid to debate COVID Vaccine Safety?
Guest Post by Steve Kirsch Recently, both the FDA and CDC advisory panels have voted to approve COVID vaccine booster shots for certain groups of people. I believe that that vote was a mistake. The…
www.theburningplatform.com
Why are the FDA and CDC advisory panel members so afraid to debate COVID Vaccine Safety?
Guest Post by Steve Kirsch
Recently, both the FDA and CDC advisory panels have voted to approve COVID vaccine booster shots for certain groups of people.
I believe that that vote was a mistake. They should have voted to stop the vaccines entirely and replace it with early treatment protocols since such protocols are safer and more effective than the vaccines. Instead, they completely avoided talking about the issue in their meetings and they refused all reasonable attempts to be challenged on what the science actually shows.
How we got here
Let’s recap a quick history of how I came to this conclusion.In early May, my friends reported death and disability after being vaccinated. I started looking at the data and the more I looked, the more troubled I became. I arranged to tell the world what I learned on Bret Weinstein’s Darkhorse Podcast with my friend Robert Malone. That video went viral with almost 1M views before YouTube censored it. Here is the one hour version.
Fast forward to September 17, 2021. I spoke out about the vaccines in the public input section of the FDA advisory meeting. I said that everyone was avoiding the elephant in the room: that the vaccines kill more people than they save. Nobody on the panel was paying attention to my talk. This is pretty typical. I wasn’t offended. But the public was listening and I got millions of impressions on my talk. No one in the mainstream media contacted me to challenge my statement.
New results show two stopping conditions were triggered
After the meeting, I did some additional research (summarized here) and I discovered that two stopping conditions have been triggered:- The vaccines have killed over 150,000 Americans. I verified this 7 different ways.
- The vaccines kill more people than they save for all age groups
I have attempted to point this out to the panel in multiple emails which I’ve posted to my Gab account.
I offered to share the original research. No interest.
I offered to share the studies published in peer-reviewed medical journals backing up what I found. No interest.
Next, I offered to donate to their research if they would debate a team of scientists on the two stopping conditions. They could name any donation amount they wanted to make it worth their time. No interest.
I pointed out that 100% of the hundreds of people I surveyed wanted to see an open debate on this as soon as possible (and not see the debate happen in slow motion in the scientific literature). No interest.

America wants a debate ASAP. The CDC and FDA committee members refuse to discuss this. They won’t debate my team under any conditions.
And I even named the team:
- Jessica Rose
- Mathew Crawford
- Chris Martenson
- Bret Weinstein
- Byram Bridle
- Myself
At this point, I must conclude that this is a tacit admission that we are right about our two stopping conditions being triggered and that the vaccines should be immediately halted.
The message that the committee is sending to America could not be more clear:

Summary
One of our team members sent me this message after my final message to the committee members asking them to debate the key issues.We really need to call out these people and make it as public as possible that they refuse to talk based on the science. The public does not need a deep understanding of the science. If they see that we have our team of gladiators in the arena and no other team in the entire world is willing to step in, that will speak volumes. Even those who are firmly entrenched on the other side will have to start asking why their champions are showing such cowardice.
You underestimate the mental retardation of most of America and the world. They don't have to debate. Their minions are tokd not to question and they DO NOT QUESTION.Why are the FDA and CDC advisory panel members so afraid to debate COVID Vaccine Safety?
Guest Post by Steve Kirsch Recently, both the FDA and CDC advisory panels have voted to approve COVID vaccine booster shots for certain groups of people. I believe that that vote was a mistake. The…www.theburningplatform.com
Why are the FDA and CDC advisory panel members so afraid to debate COVID Vaccine Safety?
Guest Post by Steve Kirsch
Recently, both the FDA and CDC advisory panels have voted to approve COVID vaccine booster shots for certain groups of people.
I believe that that vote was a mistake. They should have voted to stop the vaccines entirely and replace it with early treatment protocols since such protocols are safer and more effective than the vaccines. Instead, they completely avoided talking about the issue in their meetings and they refused all reasonable attempts to be challenged on what the science actually shows.
How we got here
Let’s recap a quick history of how I came to this conclusion.
In early May, my friends reported death and disability after being vaccinated. I started looking at the data and the more I looked, the more troubled I became. I arranged to tell the world what I learned on Bret Weinstein’s Darkhorse Podcast with my friend Robert Malone. That video went viral with almost 1M views before YouTube censored it. Here is the one hour version.
Fast forward to September 17, 2021. I spoke out about the vaccines in the public input section of the FDA advisory meeting. I said that everyone was avoiding the elephant in the room: that the vaccines kill more people than they save. Nobody on the panel was paying attention to my talk. This is pretty typical. I wasn’t offended. But the public was listening and I got millions of impressions on my talk. No one in the mainstream media contacted me to challenge my statement.
New results show two stopping conditions were triggered
After the meeting, I did some additional research (summarized here) and I discovered that two stopping conditions have been triggered:
The most troubling thing to the panel members is that both stopping conditions are now validated in the peer reviewed scientific literature.
- The vaccines have killed over 150,000 Americans. I verified this 7 different ways.
- The vaccines kill more people than they save for all age groups
I have attempted to point this out to the panel in multiple emails which I’ve posted to my Gab account.
I offered to share the original research. No interest.
I offered to share the studies published in peer-reviewed medical journals backing up what I found. No interest.
Next, I offered to donate to their research if they would debate a team of scientists on the two stopping conditions. They could name any donation amount they wanted to make it worth their time. No interest.
I pointed out that 100% of the hundreds of people I surveyed wanted to see an open debate on this as soon as possible (and not see the debate happen in slow motion in the scientific literature). No interest.
America wants a debate ASAP. The CDC and FDA committee members refuse to discuss this. They won’t debate my team under any conditions.
And I even named the team:
Let’s be very clear: no researcher would refuse a $1M academic research grant for a two hour debate unless they were hiding something very serious.
- Jessica Rose
- Mathew Crawford
- Chris Martenson
- Bret Weinstein
- Byram Bridle
- Myself
At this point, I must conclude that this is a tacit admission that we are right about our two stopping conditions being triggered and that the vaccines should be immediately halted.
The message that the committee is sending to America could not be more clear:
Summary
One of our team members sent me this message after my final message to the committee members asking them to debate the key issues.
We really need to call out these people and make it as public as possible that they refuse to talk based on the science. The public does not need a deep understanding of the science. If they see that we have our team of gladiators in the arena and no other team in the entire world is willing to step in, that will speak volumes. Even those who are firmly entrenched on the other side will have to start asking why their champions are showing such cowardice.
cubrock
Swell guy
2A Bourbon Hound 2024
2A Bourbon Hound OG
Charter Life Member
Benefactor
Multi-Factor Enabled
Anyone wanna take bets on whether the “vaccine” she took was really just saline solution?
Oh look, the statist enforcers are out.
Back the blue! /s
 www.zerohedge.com
www.zerohedge.com
The Ohio State Highway Patrol (OSHP) is preparing for a possible disruption Monday morning during rush hour of truck drivers shutting down parts of the interstate in protest over mask and vaccine mandates, according to local news Fox 19.
Dubbed the "#patrioshutdown," the movement has spread on various social media platforms and is expected to begin Monday morning and last for several hours on a stretch of highway in Ohio.
"The Patrol is aware and monitoring the situation closely to ensure roadways are safe to travel. For security reasons we cannot go into further detail at this time," Sgt. Christina Hayes with OSHP.
Hamilton County Prosecutor Joe Deters said any trucker that takes part in the expected protested today with be charged with a felony:
Back the blue! /s
Zerohedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
www.zerohedge.com
The Ohio State Highway Patrol (OSHP) is preparing for a possible disruption Monday morning during rush hour of truck drivers shutting down parts of the interstate in protest over mask and vaccine mandates, according to local news Fox 19.
Dubbed the "#patrioshutdown," the movement has spread on various social media platforms and is expected to begin Monday morning and last for several hours on a stretch of highway in Ohio.
"The Patrol is aware and monitoring the situation closely to ensure roadways are safe to travel. For security reasons we cannot go into further detail at this time," Sgt. Christina Hayes with OSHP.
Hamilton County Prosecutor Joe Deters said any trucker that takes part in the expected protested today with be charged with a felony:
Truck drivers aren't the only ones furious with their employers' decision to enforce a vaccine mandate. Federal workers just recently sued the Biden administration over the vaccine mandate."My office has learned there are plans to shut down the highways, nationwide, on Monday to protest vaccine mandates.
I want to be perfectly clear. Anyone who attempts to shut down the highways in Hamilton County will be removed from their vehicles, charged with felony Disrupting Public Services, and they will go to jail.
To those who claim to be supportive of law enforcement - law enforcement is not with you. This would pose a serious danger for our first responders and the community at large.
I have always been supportive of a citizen's First Amendment right to protest. But, this is not lawful and it is reckless. It will not be tolerated."

TINCANBANDIT
New Member
Great to see so many patriots have seen the light.....I take heed from those hippies that came before me....ALWAYS QUESTION THE MOTIVES OF THE GOVERNMENT
This was not a pandemic, nothing was to be feared, I knew this early on when we witnessed Democrat lawmakers ignoring their own warnings and mandates, they knew all along this was nothing to fear (no more so that the regular flu).
Never getting the vaccine or any others for that matter, I don't trust those in authority anymore...
This was not a pandemic, nothing was to be feared, I knew this early on when we witnessed Democrat lawmakers ignoring their own warnings and mandates, they knew all along this was nothing to fear (no more so that the regular flu).
Never getting the vaccine or any others for that matter, I don't trust those in authority anymore...
Last edited:
cubrock
Swell guy
2A Bourbon Hound 2024
2A Bourbon Hound OG
Charter Life Member
Benefactor
Multi-Factor Enabled
Oh look, the statist enforcers are out.
Back the blue! /s
Zerohedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
The Ohio State Highway Patrol (OSHP) is preparing for a possible disruption Monday morning during rush hour of truck drivers shutting down parts of the interstate in protest over mask and vaccine mandates, according to local news Fox 19.
Dubbed the "#patrioshutdown," the movement has spread on various social media platforms and is expected to begin Monday morning and last for several hours on a stretch of highway in Ohio.
"The Patrol is aware and monitoring the situation closely to ensure roadways are safe to travel. For security reasons we cannot go into further detail at this time," Sgt. Christina Hayes with OSHP.
Hamilton County Prosecutor Joe Deters said any trucker that takes part in the expected protested today with be charged with a felony:
Truck drivers aren't the only ones furious with their employers' decision to enforce a vaccine mandate. Federal workers just recently sued the Biden administration over the vaccine mandate.
Hamilton County Prosecutor Joe Deters is a Republican.
cubrock
Swell guy
2A Bourbon Hound 2024
2A Bourbon Hound OG
Charter Life Member
Benefactor
Multi-Factor Enabled
I can't believe how much sense Russell Brand makes these days, how much I agree with him, and how much I like him. I used to think him a brainless celeb. I was wrong. And, for the record, he and I would have a lot of disagreements, but we could disagree respectfully and still be friends.
Oh look, the statist enforcers are out.
Back the blue! /s
Zerohedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
The Ohio State Highway Patrol (OSHP) is preparing for a possible disruption Monday morning during rush hour of truck drivers shutting down parts of the interstate in protest over mask and vaccine mandates, according to local news Fox 19.
Dubbed the "#patrioshutdown," the movement has spread on various social media platforms and is expected to begin Monday morning and last for several hours on a stretch of highway in Ohio.
"The Patrol is aware and monitoring the situation closely to ensure roadways are safe to travel. For security reasons we cannot go into further detail at this time," Sgt. Christina Hayes with OSHP.
Hamilton County Prosecutor Joe Deters said any trucker that takes part in the expected protested today with be charged with a felony:
Truck drivers aren't the only ones furious with their employers' decision to enforce a vaccine mandate. Federal workers just recently sued the Biden administration over the vaccine mandate.
They should just park their trucks on the side of the road and block the highway by walking down the middle of it. That seemed to work for the BLM protests?


The CEO of the pharmaceutical giant Pfizer says that normal life will return within a year, but not for those who don’t have regular COVID-19 vaccinations.
During an appearance on ABC This Week with George Stephanapoulos, Albert Bourla was asked about when he foresaw the end of the pandemic.
“Within a year, I think we will be able to come back to normal life,” said Bourla, although he made it very clear that this statement only applies to those who are prepared to take regular coronavirus booster shots.
“I don’t think that this means that variants will not be continuing coming,” Bourla added. “And I don’t think that this means that we should be able to live our lives without having vaccinations, basically.”
Bourla said that the “most likely scenario” was “annual re-vaccinations” due to the emergence of “new variants.”
The Pfizer’s CEO’s comments on annual vaccinations are interesting given that the FDA has so far only approved booster shots for elderly people and “high risk individuals.”
Bourla’s rhetoric is similar to that espoused by Moderna CEO Stephane Bancel, who said last week that even younger people will have to get vaccine booster shots at least once every three years.
This once again underscores how a two tier society is being created where only those who submit to regular shots will be able to enjoy a relatively normal lifestyle.
For those who continue to refuse to be vaccinated, travel, employment and potentially even basic leisure activities will continue to be curtailed, leaving them in a de facto state of lockdown indefinitely.